
I took 10 000IU of Vitamin D3 daily, here’s what went wrong
January 20, 2026

Vitamin D3 supplementation isn’t as straightforward as it seems. I want to start with a real example. A friend of mine was taking very high doses of vitamin D3—around 12,000 IU per day—and started experiencing severe muscle spasms. I had the same issue when I was taking 10,000 IU daily. It felt like something was moving under the skin in my leg, and the spasms were visibly obvious. At first, we assumed this was a direct side effect of vitamin D, but the real issue turned out to be magnesium deficiency.
If you then take some magnesium they might not stop since vitamin D intake is too large and it continues to use up all your magnesium in the system. You need to make sure the magnesium intake corresponds to Vitamin D intake.
Even if your vitamin D blood levels look fine, magnesium is essential because it activates vitamin D in the liver and kidneys. Research confirms that all enzymes involved in vitamin D metabolism require magnesium as a cofactor—meaning without adequate magnesium, vitamin D remains inactive and ineffective regardless of how much you supplement [1][2]. High doses of vitamin D significantly increase your body’s demand for magnesium, and a deficiency can lead to muscle cramps, spasms, and even heart palpitations—exactly what both my friend and I experienced.
Calcium
Calcium is another important part of the equation. Vitamin D increases calcium absorption from food, which is beneficial for bone health. However, if calcium intake is low, the body may pull calcium from bones. And when magnesium or vitamin K2 levels are insufficient, calcium can be deposited in the wrong places—such as arteries, kidneys, or joints instead of bones. This is why taking large amounts of vitamin D on its own isn’t always safe.
Vitamin K2
Vitamin K2 acts like a traffic director for calcium, guiding it into bones and away from soft tissues. Without enough K2, calcium can become misdirected even if vitamin D and calcium intake are high. Research shows that vitamin K2 activates matrix Gla-protein (MGP), considered the strongest known inhibitor of vascular calcification [5][6]. Observational studies like the Rotterdam Study found that high dietary vitamin K2 intake (at least 32 mcg per day) was associated with a 50% reduction in arterial calcification [7]. However, recent randomized controlled trials have shown mixed results—some studies found no benefit for aortic valve calcification, though there were hints of potential benefits for coronary arteries [8][9]. For people using higher doses of vitamin D3, experts commonly recommend 100–200 micrograms of vitamin K2 per day, preferably in the MK-7 form.
Optimal levels
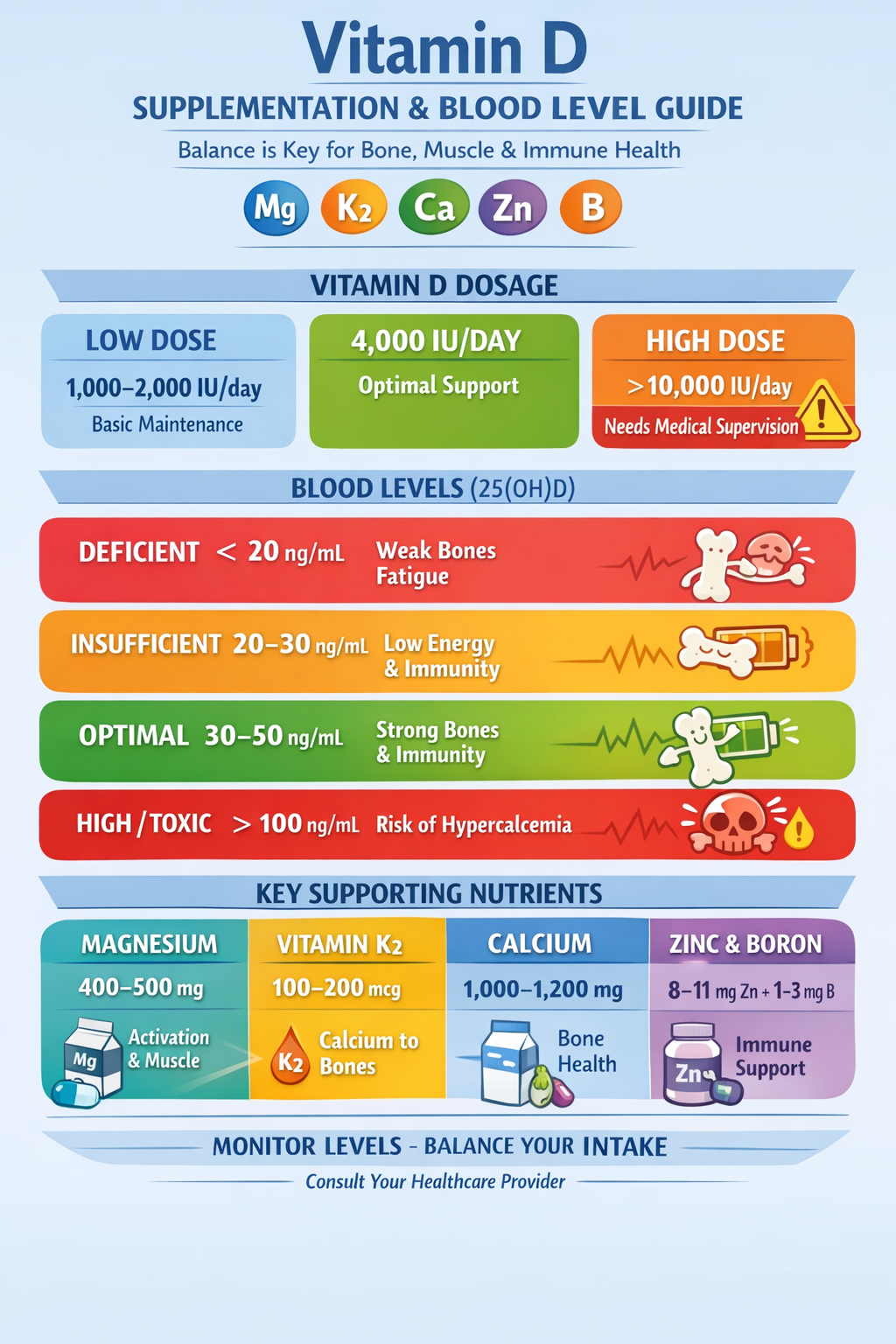
Vitamin D optimal blood levels are generally between 30 and 50 nanograms per milliliter. Levels below 20 are considered deficient, while 20–30 is insufficient. The Endocrine Society recommends maintaining levels above 30 ng/mL for optimal health, though there’s ongoing debate about the ideal range [10][11]. Staying within the optimal range supports bone health, muscle function, immune health, and proper calcium regulation. Excessively high levels—often from mega-dose supplementation—can lead to calcium imbalance and kidney stress.
What about high-hose vitamin D for severe deficiency?
If you’re severely deficient in vitamin D (below 20 ng/mL), you might wonder whether taking very high doses like 10,000-12,000 IU daily is safe or effective. Here’s what the research shows:
The Safety Ceiling for Daily Use
The highest daily dose that has been studied long-term is 10,000 IU per day. A three-year study of 373 healthy adults found that 10,000 IU daily was generally safe, though it increased the risk of hypercalciuria (excess calcium in urine) compared to lower doses [18]. Importantly, there is no research validating 12,000 IU or higher as safe for daily use—this is why I experienced those severe muscle spasms.
The Medical Standard: Weekly High-Dose Protocol
Instead of taking extremely high daily doses, the standard medical approach for correcting severe vitamin D deficiency is:
- Loading Phase: 50,000 IU of vitamin D once weekly for 8-12 weeks [19][20]
- Maintenance: Either 50,000 IU every other week, or 2,000-4,000 IU daily [21]
This weekly dosing approach (which equals about 7,143 IU daily) has been used safely for up to 6 years in some patients and is more effective than trying to take the equivalent amount spread across daily doses [22]. Some studies have even used 50,000 IU three times per week for 6 weeks to correct severe deficiency, with excellent results and no toxicity [23].
Why Weekly Dosing May Be Better
Research suggests that the total cumulative dose matters more than the frequency of dosing. A minimum total dose of 600,000 IU over several weeks is typically needed to raise levels above 30 ng/mL in deficient individuals [24]. Whether you take this as daily or weekly doses, the outcome is similar—but weekly dosing is easier to remember and may have a better safety profile.
Critical Safety Point for High Doses
If you’re taking any dose above 4,000 IU daily, you absolutely must increase your magnesium intake proportionally:
- For 5,000-6,000 IU daily: 400-500 mg magnesium
- For 10,000 IU daily: 500-600 mg magnesium
- For 50,000 IU weekly: 400-500 mg magnesium daily throughout the week
- Always include: 200 mcg vitamin K2 (MK-7 form)
Studies show that high-dose vitamin D without adequate magnesium can induce severe magnesium depletion—this is exactly what happened to me and my friend [25].
My Recommendation
If you’re severely deficient, work with your doctor on a proper loading protocol rather than self-prescribing very high daily doses. The standard 50,000 IU weekly for 8-12 weeks is safer, better studied, and just as effective as taking 7,000-10,000 IU daily—without the same risk of mineral imbalances.
You might ask, but sunlight gives way more Vitamin D3, how is that not affecting mineral levels? Sunlight is generally safer than high-dose supplementation because the body can self-regulate vitamin D production through the skin. Research shows that once enough vitamin D3 is produced from sun exposure, continued UV exposure causes its photodegradation into inactive compounds, naturally preventing overproduction [12][13]. Supplements bypass this natural control mechanism, which is why excessive doses carry greater risk.
For most adults, staying under 4,000 IU of vitamin D per day without medical supervision is considered safe. Make sure you get enough magnesium from foods like leafy greens, nuts, and seeds, or from supplements. Include vitamin K2 in the MK-7 form, aim for 1,000–1,200 milligrams of calcium daily from food, and consider zinc and boron if your diet is low in these nutrients. However you most likely get these nutrients from food anyway. If you’re using higher doses, regular blood testing is important to keep everything balanced.
Should You Split Your Vitamin D Throughout the Day?
You might wonder if it’s better to take vitamin D in smaller doses spread throughout the day rather than all at once. The short answer is: it doesn’t really matter. Vitamin D3 is fat-soluble, which means it gets stored in your body’s fat tissue and liver, then released gradually over time. Whether you take 2,000 IU once in the morning or split it into two 1,000 IU doses won’t significantly affect your blood levels or how your body uses it.
That said, taking your vitamin D with a meal containing fat helps with absorption, so consistency matters more than timing. The same principle applies to magnesium—while some people find splitting magnesium into two doses helps with absorption and reduces digestive discomfort, it’s not strictly necessary. The key is making sure your total daily intake of both nutrients is adequate and balanced. Focus on getting enough magnesium to support whatever dose of vitamin D you’re taking, rather than worrying too much about when exactly you take them.
What About Kids and Vitamin D Supplements?
Children absolutely can benefit from vitamin D supplementation, especially if they live in northern climates, spend most of their time indoors, or have darker skin that produces less vitamin D from sunlight. However, their needs are quite different from adults. For infants up to 12 months, 400 IU per day is typically recommended [14][15]. Children aged 1–18 generally need around 600–1,000 IU daily, though some pediatricians recommend up to 1,000–2,000 IU during winter months or for children with known deficiency [16][17].
The same cofactor principles apply to children—they need adequate magnesium, calcium, and vitamin K2 for vitamin D to work properly and safely. Fortunately, if children are eating a balanced diet with dairy products, leafy greens, nuts, and whole grains, they’re likely getting these nutrients naturally. Liquid vitamin D3 drops are convenient for younger children and can be mixed into food or drinks. Just as with adults, more isn’t better—excessive vitamin D in children can lead to calcium imbalance and kidney problems. Always consult with a pediatrician before starting supplements, especially if your child has any health conditions or is taking other medications. Regular blood testing isn’t usually necessary for healthy children on standard doses, but it may be recommended if higher doses are prescribed.
Vitamin D3 is fat-soluble, so it’s best taken in oil-based capsules, such as those containing fish oil or MCT oil. Magnesium glycinate is a well-absorbed form of magnesium and often easier on the stomach.
The main takeaway is this: more vitamin D3 is not always better. Magnesium and vitamin K2 are essential for it to work safely and effectively. Paying attention to these cofactors—and monitoring your levels—can help you supplement wisely without unwanted side effects.
Other nutrients that support vitamin D function
While magnesium, calcium, and K2 are the primary cofactors, other nutrients also help vitamin D work effectively:
-
Zinc: supports vitamin D receptor function and immune signaling.
-
Boron: minor but helpful in magnesium and vitamin D metabolism.
-
Phosphorus: works with calcium for bone mineralization.
Risks and symptoms of high-dose vitamin D
Taking vitamin D far above typical doses (for example, 12,000–20,000 IU/day) can increase magnesium and calcium demands dramatically. Without proper support, common symptoms include:
-
Muscle spasms or cramps
-
Heart palpitations
-
Fatigue and headaches
-
Tingling or twitching
These symptoms often indicate magnesium depletion, even if blood calcium appears normal. Over time, high-dose vitamin D without proper nutrient balance can also affect bone strength and vascular health.
The calculator below is showing the Magnesium and K2 values depending on D3 values. The labels behind are showing if the value is over or below recommended daily value
Sun-made vitamin d vs supplements
It’s important to note that vitamin D made naturally from sunlight is generally safer than taking very high doses as a supplement, even if the total IU is similar:
-
Sunlight: the body self-regulates production. After a certain point, the skin stops making more vitamin D, preventing sudden spikes in blood levels. Magnesium and K2 demand increases gradually, giving the body time to adapt.
-
Supplements: high doses bypass the body’s control. Taking 20,000 IU daily can raise blood vitamin D rapidly, creating sudden magnesium and K2 strain, which can lead to muscle cramps, calcium misdirection, or other side effects.
Even if you split the dose throughout the day, supplements still accumulate in fat tissue and continue to increase vitamin D levels. The risk comes from total daily and cumulative intake, not just one portion.
Practical guidelines for safe supplementation
If you are taking high-dose vitamin D (or planning to):
-
Moderate your dose: for most adults, 4,000 IU/day is the upper safe limit without medical supervision.
-
Ensure magnesium intake: 400–500 mg/day from food and/or supplements like glycinate or citrate.
-
Include vitamin K2: 100–200 mcg/day (MK-7 form) with your D3 dose.
-
Monitor calcium intake: aim for 1,000–1,200 mg/day total from food.
-
Support with zinc and boron if diet is inadequate.
-
Check blood levels: 25(OH)D, magnesium, and calcium after a few months to ensure balance.
Comparison of Sun-Made vs Supplement Vitamin D
| Factor | Sun-made Vitamin D | High-dose Supplement (e.g., 20,000 IU/day) |
|---|---|---|
| Vitamin D production | Gradual, self-regulated by the skin | Rapid, bypasses natural control |
| Blood 25(OH)D rise | Moderate, within safe range | Sudden, may reach high levels quickly |
| Magnesium demand | Gradual, usually met by diet | High, may exceed dietary intake → muscle cramps/spasms |
| Vitamin K2 demand | Gradual, lower risk of misdirected calcium | High, insufficient K2 increases risk of calcium deposition in soft tissues |
| Calcium absorption | Balanced, low risk of soft tissue accumulation | Rapid, higher risk if K2 or magnesium is insufficient |
| Risk of toxicity | Very low, even with long sun exposure | Moderate to high if unsupervised, long-term supplementation |
| Practical takeaway | Safe, body-regulated, minimal nutrient strain | Should only be done under medical supervision with magnesium/K2 support |
Sample Balanced Daily Routine for 4,000 IU D3
| Nutrient | Dose | Form | Notes |
|---|---|---|---|
| Vitamin D3 | 4,000 IU | Cholecalciferol | With largest meal containing fat |
| Magnesium | 400–500 mg | Glycinate, Citrate, or Malate | Split dose morning/evening |
| Vitamin K2 | 100–200 mcg | MK-7 | Same meal as D3 |
| Calcium | 500–600 mg per dose | Food preferred | Total 1,000–1,200 mg/day |
| Zinc | 8–11 mg | Picolinate or Citrate | With food |
| Boron | 1–3 mg | Optional | Via diet or supplement |
References
[1] Role of Magnesium in Vitamin D Activation and Function
https://pubmed.ncbi.nlm.nih.gov/29480918/
[2] Magnesium status and supplementation influence vitamin D status and metabolism
https://pmc.ncbi.nlm.nih.gov/articles/PMC6693398/
[3] Treating Vitamin D Deficiency and Insufficiency in Chronic Neck and Back Pain and Muscle Spasm
https://pmc.ncbi.nlm.nih.gov/articles/PMC6730953/
[4] Muscle Cramps Do Not Improve With Correction of Vitamin D Insufficiency
https://pubmed.ncbi.nlm.nih.gov/29357208/
[5] Highlighting The Substantial Body Of Evidence Confirming The Importance Of Vitamin K2
https://pmc.ncbi.nlm.nih.gov/articles/PMC7238900/
[6] Vitamin K supplementation and vascular calcification: systematic review and meta-analysis
https://www.frontiersin.org/journals/nutrition/articles/10.3389/fnut.2023.1115069/full
[7] Highlighting The Substantial Body Of Evidence (Rotterdam Study details)
https://pmc.ncbi.nlm.nih.gov/articles/PMC7238900/
[8] Vitamin K2 and D in Patients With Aortic Valve Calcification: RCT
https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.121.057008
[9] Effects of Vitamin K2 and D Supplementation on Coronary Artery Disease
https://www.jacc.org/doi/10.1016/j.jacadv.2023.100643
[10] Consensus Statement on Vitamin D Status Assessment and Supplementation
https://academic.oup.com/edrv/article/45/5/625/7659127
[11] The Optimal Protective 25-Hydroxyvitamin D Level for Different Health Outcomes
https://pmc.ncbi.nlm.nih.gov/articles/PMC12029153/
[12] Sunlight regulates the cutaneous production of vitamin D3 by causing its photodegradation
https://pubmed.ncbi.nlm.nih.gov/2541158/
[13] Sunlight and Vitamin D: A global perspective for health
https://pmc.ncbi.nlm.nih.gov/articles/PMC3897598/
[14] Vitamin D for Babies, Children & Adolescents – AAP
https://www.healthychildren.org/English/healthy-living/nutrition/Pages/vitamin-d-on-the-double.aspx
[15] Vitamin D Supplements: What Parents Should Know
https://www.chop.edu/news/health-tip/vitamin-d-supplements-what-parents-should-know
[16] Vitamin D Supplementation in Infants, Children, and Adolescents
https://www.aafp.org/pubs/afp/issues/2010/0315/p745.html
[17] Vitamin D in pediatric age: Current evidence, recommendations, and misunderstandings
https://pmc.ncbi.nlm.nih.gov/articles/PMC10060648/
[18] Safety of High-Dose Vitamin D Supplementation (10,000 IU for 3 years)
https://pubmed.ncbi.nlm.nih.gov/31746327/
[19] Treatment with 50,000 IU Vitamin D2 Every Other Week
https://pubmed.ncbi.nlm.nih.gov/22440989/
[20] Vitamin D 50000 IU Treatment Duration for Severe Deficiency
https://www.droracle.ai/articles/260342/
[21] 6-year 50,000IU/Week Vitamin D Well Tolerated
https://www.rejuvenation-science.com/research-news/vitamin-d-1/n-vitamin-d-rda2
[22] Vitamin D Deficiency in Adults: When to Test and How to Treat
https://pmc.ncbi.nlm.nih.gov/articles/PMC2912737/
[23] Evaluation of Vitamin D Repletion Regimens (50,000 IU 3x/week)
https://pmc.ncbi.nlm.nih.gov/articles/PMC2683376/
[24] Vitamin D Deficiency in Adults: When to Test and How to Treat (600,000 IU total)
https://pmc.ncbi.nlm.nih.gov/articles/PMC2912737/
[25] Magnesium status and supplementation influence vitamin D status and metabolism
https://pmc.ncbi.nlm.nih.gov/articles/PMC6693398/

